
We are currently experiencing an increasing mental-health burden in our society. According to the CDC (Center for Disease Control), in 2015, suicide was the 3rd leading cause of death in children ages 10-14, and the 2nd leading cause of death in those ages 15-34. Additionally, in just ten years’ time (from 2005 to 2015), the number of suicides in the age range of 10-14 increased by more than 51%, and by more than 35% in age groups 15-34.[1], [2] In fact, suicide rates have increased in all age groups since 1999, except for those over age 75, with exponential rates of increase after 2006. Today, suicide is now the 10th leading cause of death overall in the US.[3]
The use of psychotropic medications suggests a similar problem with regard to general mental-health. Hereto we see an exponential rate of increased use, with no signs of abatement. As reported by the CDC, “Antidepressants were the third most common prescription drug taken by Americans of all ages in 2005–2008 and the most frequently used by persons aged 18–44 years. From 1988–1994 through 2005–2008, the rate of antidepressant use in the United States among all ages increased nearly 400%.”[4]
In Robert Whitaker’s book: Anatomy of An Epidemic: Magic Bullets, Psychiatric Drugs, and the Astonishing Rise of Mental Illness in America, the IRE (Investigative Reporters and Editors) 2010 Book Award winner for best investigative journalism, Whitaker shares that in 1987, the year the FDA approved Prozac, “there were 1.25 million people receiving an SSI or SSDI payment because they were disabled by mental illness, or 1 in every 184 Americans. . . . over the next two decades the number of disabled mentally ill on the SSI and SSDI rolls soared to 3.97 million. In 2007, the disability rate was 1 in every 76 Americans, more than double the rate in 1987.” It is further reported that in 1987, “there were 16,200 children under eighteen years of age who received an SSI payment because they were disabled by a serious mental illness. . . . But starting in 1990, the number of mentally ill children began to rise dramatically, and by the end of 2007, there were 561,569 such children on the SSI disability rolls. In the short span of twenty years, the number of disabled mentally ill children rose thirty-five fold.”[5]
The rate of increase in diagnosed mental-health related disorders, suicide, and the use of psychotropic medications are all on the rise, and this is not likely to change until we begin addressing the root cause of such issues, and not just the symptoms, which are so often the primary targets in both psychiatric medicine and mental-health treatment.
As an LPC (Licensed Professional Counselor) who has worked with countless adolescents and adults, and facilitated more than 8,000 therapy sessions, I have always wanted to see a better world—one filled with more love and compassion—one with less hate and suffering. I believe that with few exceptions, most people who enter the helping professions want similar things. While I have personally witnessed many extraordinary transformations over the course of my career, I also have to acknowledge the deeper reality regarding what these general mental-health markers suggest, which is, overall, our collective mental-health needs are not being sufficiently met. I often wonder what, if anything, can be done to help reverse the course we are presently on. Almost two years ago now, I was reminded of one possible solution to our current mental-health crisis—something I continue to reflect on.
For most of my professional career, my practice was overflowing. In 2015, I relocated my residence and practice to a small rural community, and for the first time in over a decade, I found myself with a rather light case load. Thus, in the fall of 2016, when an opportunity to work as an at-risk counselor within two local school districts presented itself, I decided to take the opportunity. The job had me visit four schools each week, which included two middle schools and two high schools in neighboring districts. I was expected to work with as many as 16 youth across the four schools, a number that I had a strong feeling greatly underestimated the actual need for services. Unfortunately, I was correct; and by the end of my third month in that position, I had already worked with 30 students, and it was apparent that the need remained higher still.
With the help of the students, I was reminded of several solutions to our present day mental-health problems. As it were, it would be numerous conversations and a couple powerful pictures that offered some of the most important lessons (or reminders, if you will) that are necessary if we are going to make the world a more psychologically habitable place. May these lessons serve as an important and timely reminder of just how vital and necessary things such as love, connection, empathy, compassion, kindness and encouragement are for healthy psychological development.
Lesson #1: It’s Time To Put Down The Mask!
 This picture was given to me by a young boy. One particular day when he came to see me, he grabbed a pencil and a piece of paper from my desk and drew this image. Holding back tears, he said: “This is what I have to do here!” Unfortunately, he was right. And, without making some drastic changes to the way we deal with emotions in our society, not only will he have to do this in school, but for the rest of his life; that is, unless of course, he wants to risk inviting in more pain in the form of humiliation, criticism, and shame. In a recent post, “Why Are Men So Angry?,” I address this topic further.
This picture was given to me by a young boy. One particular day when he came to see me, he grabbed a pencil and a piece of paper from my desk and drew this image. Holding back tears, he said: “This is what I have to do here!” Unfortunately, he was right. And, without making some drastic changes to the way we deal with emotions in our society, not only will he have to do this in school, but for the rest of his life; that is, unless of course, he wants to risk inviting in more pain in the form of humiliation, criticism, and shame. In a recent post, “Why Are Men So Angry?,” I address this topic further.
This young boy had already been through several significant traumatic experiences in his life and things weren’t letting up. He was a very intelligent kid, but as should be expected, he was having great difficulty concentrating on his school work. This picture demonstrates not only what he was feeling as the result of his past and present life circumstances, but also from the implicit and explicit pressure he was feeling to stuff and avoid his feelings, especially in school. This was not the place to feel such things; he was there to “learn”!
I will never forget when I heard one teacher state (in reference to another student whose family life was in utter disarray): “They need to learn to put it on the shelf!” The justification for the above-mentioned comment was that, as adults, we too have to “put our feelings on the shelf” at times (perhaps suggesting this is also a necessary skill to have in life). Yes, it is true: most every adult practices this emotionally repressive way of being to some extent, as it is often unsafe to be vulnerable in much of today’s society. However, perhaps it isn’t good for us to suppress our painful emotional material in such a way, and maybe we should examine the potential consequences of such ways of being in the world.
Professionally speaking, I would argue that this phenomenon is responsible for a great number of the physical and mental illnesses we see in our world today, and there is a growing body of research to corroborate this suspicion. For starters, as described in the book The Language of Tears, by Jeffrey Kottler, a professor of counseling and educational psychology, there is reference to the work of biochemist, William H. Frey II, Ph.D., who, in his biochemical study of tears in the 1980’s found that emotional tears contain higher levels of proteins and other chemicals that build up during times of stress and thus have a different compositional structure than do the other two types of tears humans produce, which are often referred to as, continuous and irritant tears (those that keep the eyes moist, and those that flush foreign materials, toxic or noxious irritants, respectively).[6] Kottler and Frey postulate: “Similar to other body mechanisms that excrete waste products through urination, defecation, perspiration, and exhalation, emotional tears are a way to remove harmful materials. . . . it may also be that people who stop themselves from crying may be interfering with the body’s natural means of waste disposal.”[7] Additionally, around the same time Frey was conducting his research, Dr. Margaret Crepeau found that when she studied 100 men and women with stress-related disorders (50 with ulcers; 50 with colitis, an inflammation of the colon) and compared them to a healthy group of 50 individuals with similar age and life circumstances, those who were ill were more likely to regard crying as a sign of weakness or loss of control.[8] Since then, many other subsequent studies have produced similar findings.
We must then ask ourselves, “What is the cost of engaging in and/or promoting a behavior that may impede one of our innate stress mitigating mechanisms?” Certainly, without any knowledge of the literature, this young boy came to the same conclusion: retaining stress via emotional repression may be harmful, and does not serve to abate the stress one is under. Could this way of being be related, at least in part, to the ever increasing rates of depression, anxiety, and other mental-health related disorders? I suspect so, and in my opinion, we would be wise to abandon this long-held belief that emotional expression is both unnecessary and a sign of weakness (and in contrast, that suppressing such feelings is a sign of strength). We have no evidence that this is good for us, but we do have evidence to suggest the contrary.
Lesson #2: Keep Caring, Always Love, And Never Give Up!
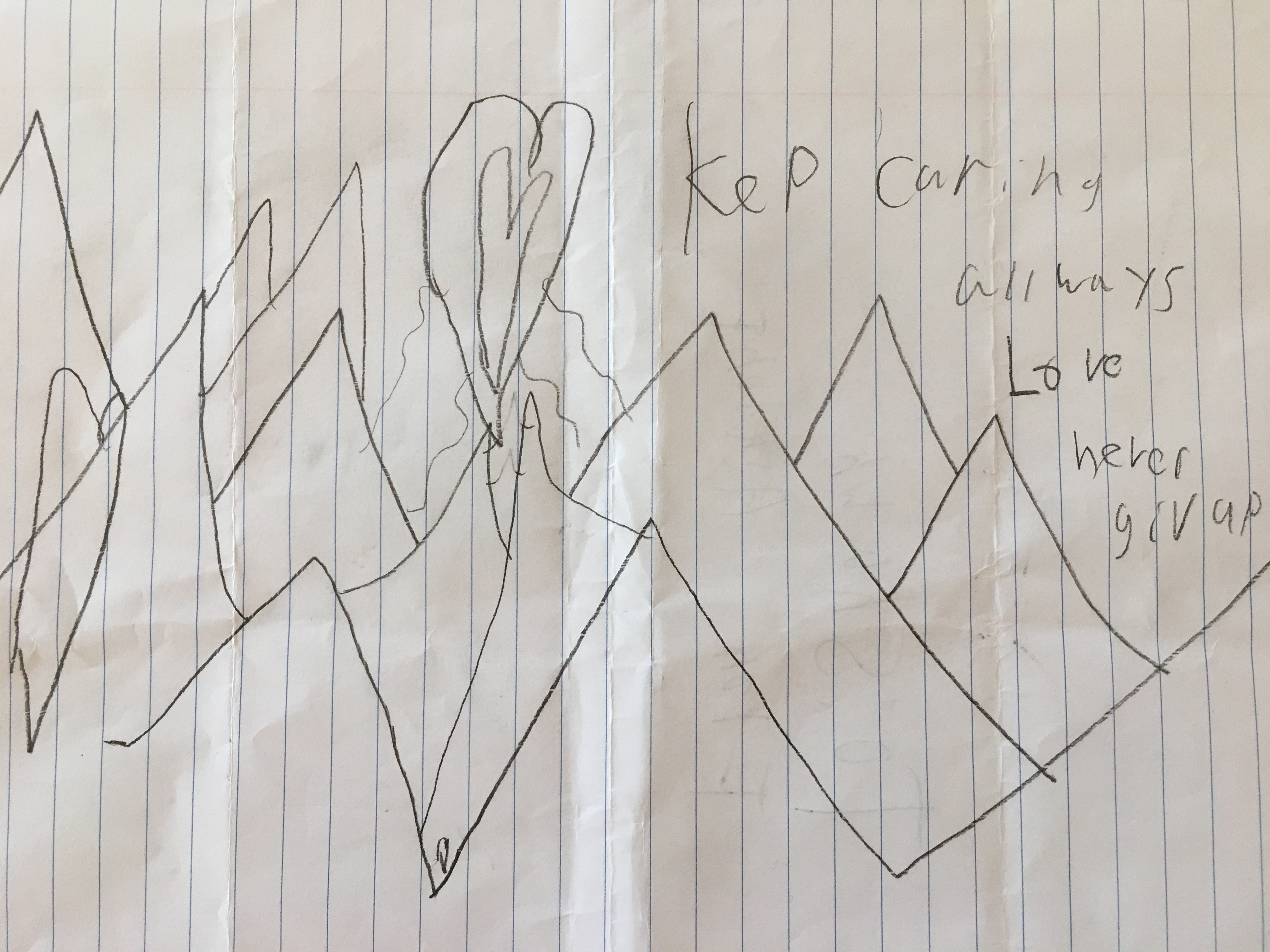 This is a picture given to me by another young boy I worked with. Similarly, he too had a difficult home life, and suffered from terrible anxiety, perhaps the worst I’ve ever experienced in someone that age. Not surprisingly, he was also struggling with his school work and was falling behind, which only perpetuated his anxiety. To motivate him, he was threatened with being held back if he didn’t get caught up, get good grades, etc.—a common practice I observed in every building I visited, and a common practice I also see many parents engage in as well. Most often, the intent behind such behaviors is a positive one: to motivate. And, I suspect that may be why behaviors supported by positive intentions are infrequently evaluated for efficacy and/or unintended consequences (something I see happening too frequently in practice). Of course, intention matters, but outcomes matter more, and we should be cautious not to evaluate outcomes solely through the lens of “intent,” in order to minimize unintended negative psychological consequences.
This is a picture given to me by another young boy I worked with. Similarly, he too had a difficult home life, and suffered from terrible anxiety, perhaps the worst I’ve ever experienced in someone that age. Not surprisingly, he was also struggling with his school work and was falling behind, which only perpetuated his anxiety. To motivate him, he was threatened with being held back if he didn’t get caught up, get good grades, etc.—a common practice I observed in every building I visited, and a common practice I also see many parents engage in as well. Most often, the intent behind such behaviors is a positive one: to motivate. And, I suspect that may be why behaviors supported by positive intentions are infrequently evaluated for efficacy and/or unintended consequences (something I see happening too frequently in practice). Of course, intention matters, but outcomes matter more, and we should be cautious not to evaluate outcomes solely through the lens of “intent,” in order to minimize unintended negative psychological consequences.
For example, this young boy was especially terrified of going to math class, where he seemed to feel the most pressure. One day, he came to see me and said he was scared about going to class. We talked for a while, and as the time came closer for the bell to ring, he began to get noticeably more and more anxious. When the bell rang—signaling the end of the period—he literally jumped out of his seat! It was only seconds later when he vomited in my trash can—a physical reaction to his overwhelming anxiety. If this is the cost of “learning,” the price is too high!
In this case, threatening the student with being held back had the positive intent to motivate; the outcome, however, was further damage to the psychological and physiological systems, not improved performance. In cases such as these, as adults and caregivers, we do not need to change our intent, but we ought to challenge ourselves to come up with alternative strategies to motivate behavior change without inflecting such collateral damage. If the stress and anxiety this student felt were mitigated first, I have no doubt that the cognitive abilities he was lacking would dramatically improve, as modern science tells us as well. There was nothing wrong with his intellectual ability, there was something wrong with his overactive nervous system, a product of his developmental and environmental experiences.
What Does The Research Suggest?
As I will often cite in my writing, and I’ve spoken about elsewhere, in 1998 perhaps one of the most important studies ever published appeared in the American Journal of Preventive Medicine, and today is most notably referred to as the “Adverse Childhood Experiences (ACE) Study.” This study was the largest epidemiological study ever conducted of its kind, and demonstrated findings unlike anything found since. As stated in this study: “The number of categories of adverse childhood exposures showed a graded relationship to the presence of adult diseases including ischemic heart disease, cancer, chronic lung disease, skeletal fractures, and liver disease.” Further, “Persons who had experienced four or more categories of childhood exposure, compared to those who had none, had 4- to 12-fold increased risks for alcoholism, drug abuse, depression and suicide attempt.” Specifically, an ACE score of 4 (out of a possible 10) correlated to a 12.2-fold increase in attempted suicide, which is to say, an increase of 1,220%![9] As, Vince Felitti, MD, FACP, primary author of the study later mentioned in a talk he gave, “With an ACE score of six or more, you can get up between a 31- and 50-fold increased risk in attempted suicide in adolescents; that’s a 3,100 to a 5,000 percent increase!” Further, “Life expectancy with an ACE score of six or more was shortened almost 20-years!”[10] In my conversations with the students I worked with, I discovered that many of them would have had an ACE score of six or more, and some who would have scored all ten items!
What helps mitigate the extreme impact of these ACE’s? Dr. Bruce Perry, M.D., Ph.D., senior fellow at the Child Trauma Academy in Houston, TX., and one of the most recognized authorities in the area of childhood development and the impact of trauma, abuse and neglect, states that what helps children get better is, “Connection to other human beings, human beings who are present, who are patient, who are kind, who are sensitive.” Perry adds, “They don’t need to be necessarily psychologically insightful; they don’t need to know anything about trauma.”[11] At a professional training I attended in the fall of 2016 with Mr. Perry, he further referenced some new data collection that is positively correlating psychosocial and intellectual improvements with positive relational support.[12]
Perry is not alone in his understanding of what promotes healing and general well-being in humans. Other internationally recognized authorities, developmental psychologist, Gordon Neufeld, Ph.D., and his co-author, medical doctor and addiction expert, Gabor Mate’ M.D., have eloquently argued in their book Hold On to Your Kids: Why Parents Need to Matter More Than Peers, that “attachment,” that is, the psychological and emotional connection between human beings, particularly in a hierarchical order (adult to child vs. child to child), is what determines everything from the health of the individual to the teachability of the student.[13] Without relationship and healthy attachment, we suffer—in every way possible!
Most recently, I happened across a video from a man by the name of Josh Shipp. In reference to being abandoned by his parents and subsequent experiences with foster care, Mr. Shipp’s motto is: “Every kid is one caring adult away from being a success story!”[14] Not only did this prove true in his life, but research is validating this claim as well. Today’s children, and this world, need it now more than ever, and this young boy intrinsically knew that when he wrote, “Keep caring; always love!”
This simple message and the research backing it may seem obvious. Further, it may seem like something most people are already doing; however, in my experience, there is often a discrepancy between the message people believe they are sending, and what the other person actually experiences. For example, when I spoke with many teachers about the importance of building relationships with their students, I was often met with the response, “We already do that,” even though I could clearly see that wasn’t always the case. This was not only evident in my clinical observations, but supported by data I discovered in a 2015 report sponsored by the Colorado Department of Health & Environment, as part of the Healthy Kids Colorado initiative. This survey covered a variety of topics from substance use, to participation in extracurricular activities. In the section on “School Protective Items,” there was the question: “Teachers care and give encouragement,” to which the score for the region I worked in (along with several other counties) was 58.5%, a failing grade by any school metric. The state-wide score was only marginally higher at 60.9%.
I predict that these scores would be very similar in most places in the world where standard western cultural values and operations have been adopted. What is often very difficult for people to recognize with regard to developing relationships, is that the solution is not in technique or skill per se. This is not entirely a problem of what one does, but rather, how one does it. Relationship building is not a skill that can been learned via the intellect alone; an empathic, emotional quality, with presence and awareness, is required. Healthy human connections occur through feelings, not through information. If we wish to engage the head, we must first engage the heart: attempting to work in the opposite order produces rather poor results and a lot of unnecessary frustration and suffering for all parties involved! The capacity for such emotional connection is an innate human ability, but it seems many people are losing that ability—likely the result of multi-generational emotional suppression. Many people now think they are connecting, instead of feeling their way to genuine connection.
What Can Be Done?
This is really a question about where a cycle of psychological dysfunction can be broken. In this context, even though most of the problems that show up in the school setting originate in the child’s home and outside experiences (as the ACE data demonstrates), when it comes to helping children heal from trauma, abuse or neglect, and helping to promote healthy psychological maturation, changes within schools may be the best option available. Dysfunction begets dysfunction, and in my clinical practice, I often find it very difficult to help promote the necessary healing and changes in parental and family systems that contain deeply ingrained patterns of trauma and abuse. In many such families, it is often difficult for members to recognize the dysfunctional patterns and ways of being they are in—for many, dysfunction is simply normal, and as such, the need for change difficult to recognize. As such, changes with regard to school culture and assessment could be a viable place to begin breaking these cycles. If schools began to focus more on psychological and developmental needs (further recognizing that healthy psychological/psychosocial development is a precursor to academic growth), and began working toward progress in these areas as well, it is highly probable that we would begin to not only see psychologically favorable results, but also the improvements in academic performance we’ve been so desperate to achieve as well.
Further, given that school is where children will spend the majority of their time with adults, it makes sense that we could get a lot of mileage from implementing practices based on the developmental needs of children, including more trauma-sensitive, adult-to-child relationship-building practices, especially for those students whose social/relational/emotional needs have not been sufficiently met. What this means is that our schools would be wise to move to a model of education that works to incorporate the developmental needs of the child. As Dr. James Comer, Maurice Falk Professor of Child Psychiatry at the Yale Child Study Center and Associate Dean at the Yale School of Medicine has stated: “In order to realize the full potential of schools and students, we must create—and adequately support—a wide and deep pool of teachers and administrators who, in addition to having thorough knowledge of their disciplines, know how children develop generally and academically and how to support that development.”[15]
What excites me most is that some schools have already successfully made this shift in their approach and culture with amazing results. The documentary film Paper Tigers is about one such school in Walla Walla, Washington, where implementing such practices led to a 90% decrease in suspensions, a 75% decrease in fights, and a 5-fold increase in graduation rates![16] I would love to see every school adopt these strategies, and for school administrations to make the necessary changes in policy to best allow for these changes to occur, as Dr. Comer and others suggest. To be sure, to best combat this issue overall, we need all capable adults across the board, in every profession, to work with our youth in a kind, compassionate, developmentally-appropriate, relationship-orientated way; however, changes to school policy, operations and objectives, would be a great place to start.
What’s At Stake Without Changes?
First, we may presently be on the fast-track to losing the trait that makes us most fundamentally human, and life worth living: access to our emotions! Once we have experienced sufficient pain, we all begin to develop defense mechanisms to numb ourselves, some internal, some external. While such strategies often help us in the short-term, the long-term trade-offs should cause us to reevaluate whether it’s worth it. When we numb and psychologically disconnect ourselves from our pain, we simultaneously begin to disconnect ourselves from accessing the positive feelings we wish to experience as well (an unintended consequence). With the employment and overuse of our current defense mechanisms, we may very well also lose access to our joy, love and happiness. No one likes to feel pain, to be scared, sad, or hurt, but these feelings are part of the human experience, with few exceptions. I propose that ultimately, as I’ve suggested earlier, suppressing these feelings long-term carries a hefty price, and only serves to exacerbate the symptoms we do not want. In the extreme, we see humans lose their capacity for love and empathy altogether. The rapid rise in extreme violence, mass shootings, etc., is a testament to that potential. You can be assured: these acts do not come from those who feel connected and loved by others!
Generally speaking, in my work with children who have been abused, neglected or maltreated, their hearts somehow remain open through about the 6th or 7th grades. As such, they remain amenable to loving connection if it becomes available. Once moved into adolescence and the high school years, I’ve witnessed rapid acceleration of emotional shut-down. Of course this varies person to person, but once the heart is closed, I find that it is very difficult to re-open, and for those this happens to, they are often more prone to seeking their attachment needs in more problematic and distorted ways. People need love and connection, and if they can’t get it in healthy ways, from healthy sources, they will seek it in unhealthy ways, and through unhealthy sources. In this regard, two more statistics from the ACE study are important to mention: with an ace score of four, there is a 2.5-fold increased risk of contracting an STD (sexually transmitted disease), and a 3.2-fold risk of having intercourse with 50 or more sexual partners; that is, a 250% and 320% increase respectively!
From these statistics we might infer a couple phenomenon not specifically mentioned in the report. First, an increased risk in STD’s would be related to a lack of protection during intercourse. Next, a lack of protection, combined with an increase in sexual partners, would likely lead to more pregnancies. Those who are emotionally wounded and shut down are present-focused (not future-focused), and are consumed with their immediate needs (and sex substitutes for genuine, unconditional love and connection in this population). They are not thinking of the future and/or the consequences of their actions (and no, the lectures do not help!).
As Abraham Maslow pointed out many years ago, planning, and future-oriented thinking does not simply happen because of “education,” it happens as the result of sufficiently meeting our lower-order needs first.[17] All the sex-education in the world will not solve such a problem, only genuine love and healthy connection will. In a myriad of ways, we cannot afford to continue offering informational solutions to emotional problems and expect to move forward. What will continue to happen if we don’t find a way to provide children a healthy way to meet their social/relational/developmental needs is, they will be capable of bringing life into the world, but not capable of providing the emotionally supportive and enriching environment needed to promote physiological and psychological well-being—and the cycle will continue—picking up momentum with every rotation.
A Call To Action
We are now living in a world riddled with deep, unresolved emotional pain: the statistics presented at the beginning speak to this. Unfortunately, this is what happens when our emotional debts have gone unpaid for far too long. Love doesn’t always equal happiness; rather, it means authentic, heart-felt interaction with one another, as raw and painful as that may be at times. In such times, we do not need advice or “words of encouragement”; in fact, speaking might be the worst thing one can do for someone in the throes of an emotionally dark time, for there truly are no words strong enough to ebb the tide of deep-felt emotion. What is called for is presence, and perhaps a compassionate touch. As the saying goes, provide a shoulder to lean on, not a “half-time motivational speech” (as a recent client shared with me regarding his interactions with a previous counselor). Love also means tolerance and patience with what is, and trust that we were born with an innate ability to heal if the conditions are right. We would not have access to our tears if they did not serve a purpose. If we replace resistance with acceptance, we have a much greater probability of getting ourselves to where it is we’re trying to go, a place impossible to reach via delusional pretending and mind-numbing chemicals (our most popularly exercised attempts to get out of psychological suffering). If nothing else, let’s first practice being kind, especially to the children we may interact with—they may be the only key to saving us from the mess we’ve created.
Before I close, I want to be very clear: I am aware that there are some incredible teachers, parents, and other caregivers out there—those who are very adept at building healthy attachment relationships. My goal in writing this piece is to both highlight how important that is, as well as to bring attention to the fact that we need more of it, as the data mentioned above suggests. I can’t imagine what improvements we might see in the world if that score for whether students felt encouraged and supported moved into even the 80% range (vs. the current 58.5% regional and 60.9% state-wide scores mentioned earlier), but I have a feeling it would be huge!
In a recent 60 Minutes interview with Oprah Winfrey and Dr. Bruce Perry, Oprah credits a 4th grade teacher for being a pivotal figure in helping her overcome the atrocities of her own childhood. From being a sexual-assault survivor to growing up in poverty, it would be the love she felt from this teacher that she credits for her success today. From this elementary teacher, Oprah learned she was of value to another human being, as a human being—a lesson far more important than any academic knowledge she could have gained during that 4th grade year.[18]
Today, more and more students who have not had their developmental/psychological needs adequately met are showing up in the classroom, and these students can be very difficult to manage. Again, I would not debate that the parents and families (again, in general) of such students should spend more time building these necessary, healthy attachment relationships with their children; yet, in today’s social and economic climate, we have to face the reality that it will be day-care providers and teachers who will likely continue to spend the greatest number of hours with children, not parents and families (even the psychologically heathy ones). As such, this could be the only safety net available for many children coming from relationally impoverished environments outside of school.
Thus, for the reasons I’ve mentioned throughout, I suggest one way we may be able to curb the rising burden of mental-health related issues in our society is through changes in our educational system. I propose that our educational system adapt to these increasing problems by restructuring what it means to demonstrate “growth and learning,” by including developmental and psychological milestones, and holding teachers accountable for the relational qualities of their classroom environment and interaction with students.
As Maslow famously pointed out, emotional growth must occur before intellectual growth, and by simply acknowledging and interacting with students differently, with more compassion and understanding, schools will likely have an easier time actually meeting the intellectual growth standards they are presently myopically focused on. There is some good news here: this won’t require more work per se, there does not need to be more administrative tasks taken on. What will be required is a new understanding—a new way of being with children (and others, of course)—one that is more compassionate, empathetic, and serves first to build the child’s sense of self-worth before their test scores.
I also realize that such changes would be more easily accomplished if those in charge of federal policy begin to support them, recognizing the current social/relational climate for what it is, and thus the need to promote a more psychologically adaptive environment through policy, education, and hiring practices. The data mentioned at the beginning of this writing speaks to a society in need of help! I propose that we heed the implicit and explicit advice given by the young people I’ve shared above: 1) let’s work to put down the mask, encouraging healthy emotional expression vs. repression, and 2) let us remember to keep caring and always love above all else! And, should it be difficult to trust the advice of such young children, let us incorporate the wisdom of published scientific studies and the advice of many leading experts in the field, as we invite schools and adults everywhere to help meet the growing psychological needs of many of today’s children, so that we may begin to make a turn towards a healthier psychological evolution.
References:
[1] National Center for Health Statistics. 10 Leading Causes of Death by Age Group, United States, 2005. Atlanta, GA: Centers for Disease Control and Prevention, 2005. https://www.cdc.gov/injury/images/lc-charts/10lc_overall_2005b-a.pdf
[2] National Center for Health Statistics. 10 Leading Causes of Death by Age Group, United States – 2015. Atlanta, GA: Centers for Disease Control and Prevention, 2015. https://www.cdc.gov/injury/wisqars/pdf/leading_causes_of_death_by_age_group_2015-a.pdf
[3] National Center for Health Statistics. Increase in Suicide in the United States, 1999-2014. Atlanta, GA: Centers for Disease Control and Prevention, 2016. https://www.cdc.gov/nchs/products/databriefs/db241.htm
[4] Pratt LA, Brody DJ, Gu Q. Antidepressant use in persons aged 12 and over: United States, 2005–2008. NCHS data brief, no 76. Hyattsville, MD: National Center for Health Statistics. 2011. https://www.cdc.gov/nchs/products/databriefs/db76.htm
[5] Whitaker, Robert. Anatomy of an Epidemic: Magic Bullets, Psychiatric Drugs, and the Astonishing Rise of Mental Health Illness in America (New York: Broadway Books, 2010), 7-8.
[6] Kottler, Jeffrey A. The Language of Tears (San Francisco: Jossey-Bass, 1996), 61-63.
[7] Kottler, Jeffrey A. The Language of Tears (San Francisco: Jossey-Bass, 1996), 63.
[8] Brody, Jane E. New York Times, Science “Biological Role of Emotional Tears Emerges Through Recent Studies,” August 31, 1982. http://www.nytimes.com/1982/08/31/science/biological-role-of-emotional-tears-emerges-through-recent-studies.html
[9] Felitti, Vincent J., Anda, Robert F., Nordenberg, Dale, Williamson, David F., Spitz, Alison M., Edwards, Valerie, Koss, Mary, Marks, James S., “Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study,” American Journal of Preventive Medicine 14, no. 4 (1998): 245-258.
[10] “ACE’s by Vincent Felitti, MD.” YouTube. Video File. December 6, 2010. https://www.youtube.com/watch?v=Me07G3Erbw8&t=1723s
[11] Post Institute for Family Centered Therapy. “Trauma, Brain & Relationship: Helping Children Heal.” YouTube. Video File. March 12, 2013. https://www.youtube.com/watch?v=jYyEEMlMMb0
[12] Perry, Bruce. “The Impact of Trauma and Neglect on the Developing Child.” Lecture, Greeley, CO, April 11, 2017.
[13] Neufeld, Gordon, and Mate’, Gabor. 2005. Hold On to Your Kids: Why Parents Need to Matter More Than Peers. (New York: Ballantine Books).
[14] Shipp, Josh. “Professional Development Speakers for Teachers: One Caring Adult.” YouTube. Video File. May 20, 2016. https://www.youtube.com/watch?v=OfWWWsrlGvs
[15] “Schools That Develop Children.” The American Prospect. Accessed May 16, 2018. http://prospect.org/article/schools-develop-children.
[16] “Overview.” Paper Tigers. Accessed April 15, 2018. https://kpjrfilms.co/paper-tigers/.
[17] “Maslow’s Hierarchy of Needs.” Wikipedia. May 01, 2018. Accessed May 05, 2018. https://en.wikipedia.org/wiki/Maslow’s_hierarchy_of_needs.
[18] 60minutes. “The “life-changing” Story Oprah Reports This Week.” YouTube. March 09, 2018. Accessed June 02, 2018. https://www.youtube.com/watch?v=dF20FaQzYUI.
[…] a previous post, What Children Can Teach…, I referenced some of the current statistics regarding our rather poor and declining […]